
(Pix (c) Larry Catá Backer 2013)
At the September 10, 2013 meeting of the University Faculty Senate, University Administrators stood for questions and presented information to the faculty assembled relating to the new Wellness Program Initiative and to their plans for its implementation. This effort in informational transparency was much appreciated by many, though some regretted that there appeared to be little effort to foster engagement transparency. The result, of course, is a somewhat awkward dialogue in which information is presented to a stakeholder governance group with the underlying implication that there is absolutely no intention of permitting further effective governance participation, even at the margins. One can get a sense of this, and the record of these efforts, from the Video record of the September 10, 2013 meeting available here. Taking that position is the University's right; but as a matter of strategy, respect for the history and traditions of shared governance and of the hard work of the last several years to restore trust, choosing to proceed in this way may produce quite regrettable and otherwise avoidable outcomes.
History will decide the consequences of administrative and policy decisions now apparently written in stone. And the Board of Trustees, as overall institutional manager, will exercise its oversight, accountability and control role. More interesting, both at Penn State and for all enterprises also considering plans like this are questions that continue to arise about the way such plans are structured and defended. Among those with more resonance were a number referencing the wellness programs focus on women's reproductive strategies and plans. (VIDEO OF MEETING RECORDING HERE) . These touch on issues of privacy, personal autonomy and respect for human rights and dignity that I have suggested may be legal in the United States but may also come close to touching on human rights detrimental actions that are the object of discussion in international human rights. (Clip of "Penn State professor questions administrators about invasion of employee privacy") There have been little by way of effort among the enterprises considering plans like this in the United States to address the international human rights norms dimensions of these plans. That is a pity; it may produce consequences.
This post and some that may follow will post questions raised (and responses if provided later)--the object is to further the sort of dialogue that might have been more profitably engaged in before policy determinations had been made, and perhaps to serve as a basis for industry leaders and the third party providers that serve them, in modeling approaches to better policy and implementation methodologies and structures.
These questions are raised by a concern for the failure to correct health care inflation to the per capita rate, and in the naive cost projections using worst case past growth and ignoring national trends in health care inflation.
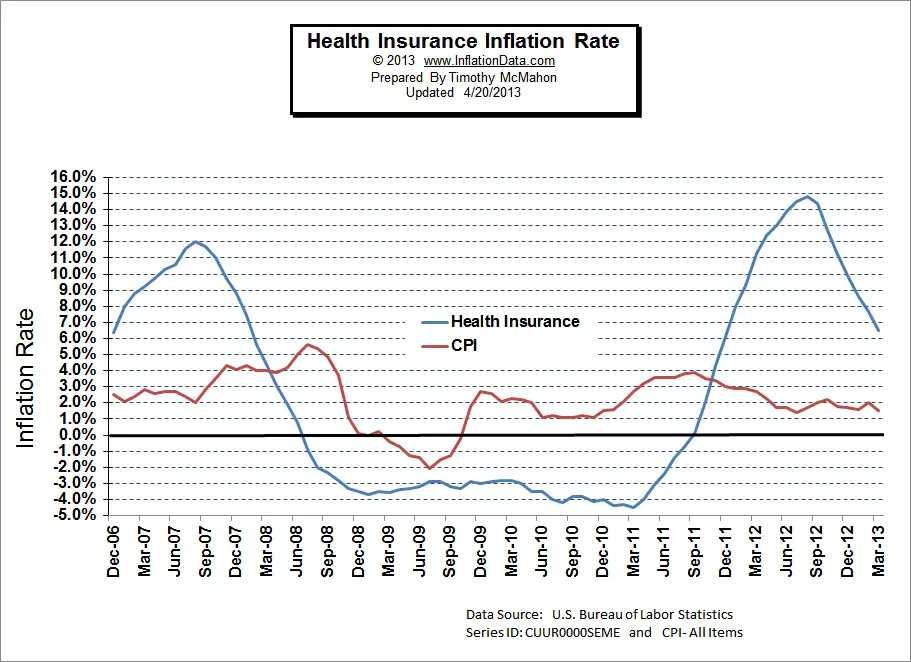
1) The table of health care costs provided in Appendix C in the Senate Agenda for Sep 10th 2013 is somewhat at odds with the broad statements made by the administration on the increase in health care costs. In particular, the PSU health care inflation for the 2008-2013 period has averaged 7.6% over the period, and only on two occasions 08-09 and 12-13 did the costs increase by more than 10% (see below). Both those years, if I recall correctly, coincided with changes in health care coverage, namely Highmark taking over as sole supplier, and the recent change in co-pays and deductibles, concurrent, I believe, with the expansion of benefits for postdoctoral researchers, which I should note will not be covered by the corresponding increase in F&A until 2014.2) The reported health care costs are gross costs, not per capita or adjusted for demographics. The number of covered employees is a matter of record (but the PSU budget Fact Book data for employment by classification is not available online for years before 2011) and the per capita adjustment is trivial and ought to be reported. The number of faculty increased 8% over the period, and I would not be surprised to learn that the number of staff increased more. Further, the employee demographics are also a matter of record, and the age profile of the employees is likely to have undergone a secular drift over the interval.3) There is a well documented _decrease_ in health care inflation underway in the US. The increase in health care costs relative to overall inflation is fairly well understood, it is driven by demographics, perverse incentives in insurance markets, increased availability of high cost treatments and the Baumol Effect. Several of those effects are saturating leading to a decrease in the rate of increase in costs. A cynical view of the estimated savings due to the Wellness initiative is that the projected decrease in the rate of increase of costs is due primarily to the overall decrease in growth of US health care costs, and stabilization of the PSU employee demographics and is completely independent of any Wellness Initiative.4) Penn State runs at about half dozen different health care programs: in particular Hershey and unionized employees are not affected and constitute a significant fraction of the Penn State covered employees. The costs, and hence projected percentage savings need to break out how many employees are covered by the different plans and how those costs have changed. This would be particularly interesting given the claimed decrease in the rate of increase of costs at Hershey after their Wellness initiative. A detailed comparison of all the different health care options would also be useful.5) More information is required about the (10 year) contract with Highmark. In particular, does Highmark receive a percentage fee or a fixed fee? Does PSU carry a capital reserve for its self-insured liabilities, or has the program been funded wholly from cash flow? How were WebMD and ICH (Tomayko Group) chosen for the screening program? What are the costs of the screening? What is WebMD paid for PHR storage and is the contract with Highmark or PSU? What third parties were consulted on the issue, and what payments were made to whom for any consultancy services by either PSU or Highmark?6) The consultation with the Senate Benefits committee was made in Oct 2011 (see appendix E), slide 6 specifically discusses a "Reward" system Wellness initiative. The very sketchy outline is quite different from that implemented currently I am also informed that the analogous presentation to the University Staff Advisory Committee was truncated partway through the presentation due to time constraints and that the Wellness initiative was not presented to the Staff. This is somewhat at odds with the presentation made by the HR office.7) Senior VP Gray mentioned the impending increase in SERS contributions as a cost factor for the University in the near future. A minority of PSU employees are SERS members, and the cost shortfall in the funding of that system is due to a combination of the State stopping employer contributions while increasing benefits in that system in an ill timed move. Are we to understand that the drive to reduce health care benefit costs for TIAA-CREF covered employees is due to the State caused shortfall in the SERS system and demand that PSU cover part of that shortfall?8) Have the Executive rank employees of Penn State done the Wellness Profile and Biometric Screening?9) What data were used to generate the estimated $4.7 million in savings in the current fiscal year from the Wellness initiative which is effective halfway through the year? Does this estimate include the fairly well known effect of a spike in health care costs when screening is done due to early discovery of health issues and short term increase in treatment costs?
Year
Gross %-delta
PSU
%-delta Employees
PSU %
Inflation Health Inflation
08 150.4 118.9 31.5 79.0 4 9
09 169.2 12.5 134.9 13.5 34.3 79.7 0 -3
10 174.8 3.3 138.4 2.6 36.4 79.2 2 -3
11 177.2 1.4 143.3 3.5 33.9 80.9 -4 1
12 193.0 8.9 161.3 12.6 31.7 83.6 3 4
13 217.0 12.4 180.2 11.7 36.8 83.0 2 9
13e 210.4 175.5 35.0 83.4
44.5 51.5
mean 7.6% mean 8.7%
08 150.4 118.9 31.5 79.0 4 9
09 169.2 12.5 134.9 13.5 34.3 79.7 0 -3
10 174.8 3.3 138.4 2.6 36.4 79.2 2 -3
11 177.2 1.4 143.3 3.5 33.9 80.9 -4 1
12 193.0 8.9 161.3 12.6 31.7 83.6 3 4
13 217.0 12.4 180.2 11.7 36.8 83.0 2 9
13e 210.4 175.5 35.0 83.4
44.5 51.5
mean 7.6% mean 8.7%

http://inflationdata.com/articles/wp-content/uploads/2013/04/Health-Insurance-Inflation-vs-cpi.jpg
{kind=link}
Staffing:
2007 5335 Faculty
2012 5762 Faculty
almost 10% at Hershey
Change: 427 Percentage Change: +8% over 5 years
2011 11832o
Faculty+Staff
2012 17619 +0.5%
2011 17533 2011 4781 Faculty 1040 Full Prof 11249 Staff 1416 Executive/Admin excluding Hershey
Here are another set of observations. These relate to the answers to the questions formulate dby the leadership of the University Faculty Senate for presentation at the Sept. 10, 2013 meeting. For my own analysis see, The
Faculty Senate and Penn State Administrators Respond to Criticisms of
the Penn State Wellness Program With My Analysis of Responses:
The administration's answers to the Senate questions about the Wellness Initiative, Appendix C of the upcoming Sept. 10 Senate Agenda, fail to give a substantial reason why additional revenue from participants is required in the upcoming plan year, and why a penalty option for getting preventative medical care rather than an incentive option is better for our self-insured community. Claiming that there was low participation in the voluntary options over the past year is not sufficient data or warrant that a penalty is necessary when the voluntary activities offered in the past carried no incentives such as waiving deductibles, or a premium discount. And their answers do not reveal the tracking that began over two years ago with Highmark and WebMD of our medical records to establish future differential costs based on our health conditions, genetic make up, or life choices. The invasion of privacy and body is likely in violation of ADA law, and law regarding an employers requirement to provide genetic material.
In the context of the Affordable Care Act, all health plans initiated after March 2010 must offer yearly preventative care including lab work at no cost to the participant--i.e. no copay or deductible. Our PSU plan is grandfathered and exempted from that, so we have and will continue to pay a $250 deductible and office visit for out preventative yearly check-up with lab work that is billed in-network at more than $300. PSU is clearly not a leader in the health care plan it offers and it's partnership with Highmark is now under question as from the remaining evidence given in the report, it looks like all of it is derived from studies done by Highmark about additional services Highmark can provide for additional costs.
I think a good question to ask is: Why not an incentive to reduce our deductible if we visit our doctor and have lab work done in that insurance year? That would show a genuine interest in our wellness within our self-insured group. In fact, there is recent large scale research showing a dramatic decrease in blood pressure when participants do not have copays: http://www.huffingtonpost.com/2013/08/21/reduce-blood-pressure-no-copay-easier-to-take-medicine_n_3789852.html
I offer the following questions to David Gray and Susan Basso regarding their answer to the sparse table of data on Penn State Health Care Cost they provide on page 5 of Appendix C, without any explanation of the data. I believe the table is sparse because they have things to hide. It is important to reference the report given by David Gray to Faculty Benefits at their April 23, 2013 meeting. Here is a quote from those minutes: "This past year PSU health care costs exceeded the previous year’s by 7.5%. In 2012, the operating margin was +1.6% as compared with 7-9% in previous years. Without Penn State Hershey, this operating margin would have been barely 0.2%. As a result, Dr. Erickson charged Susan Basso and David Gray with finding ways to reverse this trend."
http://www.senate.psu.edu/about_senate/committees/fb/12-13/minutes/fb042313min.pdf1. Are the Admin Expenses listed in the table as <5% part of the Total Health Care Costs listed in row 1, or beyond and above the Total Health Care Costs?
2. Are the Total Health Care Costs equal to the claims paid? or, the claims paid + PSU admin costs? or, the claims paid, + PSU admin costs, + the amount paid to Highmark to administer the plan?
3. If the Total Health Care Costs includes more than just the claims paid, what is the exact amount paid for claims processed? And, what is the amount paid to Highmark to administer the plan? And what costs does the administration have within the Office of Human Resources to maintain the plan? These separate costs are fully represented in the table. Why are they hidden, or not included in the table?
4. David Gray's report to Faculty Benefits committee on 4/23/13 indicates that the university had an operating margin, or surplus, of 7-9% in years prior to 2012, and an operating margin of 1.6% in 2012. Which row in the table represents the dollar amount of that operating margin? Or is that margin included in the Admin Expenses row, and if so, how can it be greater in percentage (7-9%) than the <5% indicated as Admin Expenses?
5. What has been done with the surplus funds in the operating margins of 7-9% in prior years? Where is it shown in this table, and if it is not shown, then why not
6. In the row of Employee Contributions, how much is premium, how much is copay, and how much is deductibles? The difference between these is crucial to look at how the plan has changed over the years with the introduction of higher deductibles two years ago.
7. Since we are a self-insured plan, we know all these costs and sources of income for the plan. Why isn't this table being transparent about that data?
8. Since we are a self-insured plan, should we not also be a self-governed plan, with clearly visible actions and documents that reflect shared governance? The actions and documents that currently exist do not exhibit shared decision making.
No comments:
Post a Comment